
New UK IRR17 consent - dose rate and accelerators
Published: Jul 14, 2023
[Updated October 2023 - the overall substance of this article remains valid so we are not going to make changes. However we now note that the IRR17 Consent Safety Assessment Templates from HSE are now available on the HSE website. As we thought, they are practically identical (in wording) to the ONR guidance which is discussed below. Of note, the key line discussed below, "These estimates must show that dose rates do not exceed 7.5 micro Sv/h outside any shielded enclosure" is also present in the HSE documentation, so our discussion and analysis remains the same. We are sure that once new and current consent holders have reviewed this requirement against their current documents, dose & dose rate assessments, and risk assessments, there will be plenty of calls to HSE for comment and clarification].
ONR Consent - guidance - accelerators
[Ionactive note: The matters raised in this blog entry have already been communicated to a radiation safety specialist regulator at ONR. They are looking into this issue and have said they will report back to Ionactive. In the mean time - read on!].
If you have not already seen the new IRR17 consent ONR guidance - then feel free to head over to the following page: Application for certificate of consent of specified practice(s) in accordance with Regulation 7. This will take you to the main page of the ONR resource. The specific guidance we are considering in this blog article is 'The operation of an accelerator' which can be found at the above link as a linked word document. If you want direct access then the link is as follows: The operation of an accelerator (note that this will directly download a word document).
What you are then looking for is section 4 (line 4) of a table under the heading 'Safety Assessment Content and Guidance' (which is part 2 of the guidance) - this will be found on page 4. The paragraph subject to analysis in this blog article is as follows (this has been reproduced completely, the bolded emphasise is by Ionactive).
Table section (4) of section (2) 'Safety Assessment Content and Guidance'
Applicants must provide estimates of the dose rates to which employees and others (not including patients where applicable) could be exposed during both routine operations and in the event of any reasonably foreseeable radiation accident. This will include the maximum dose rates outside any shielding to which employees and members of the public could be exposed to at each location. These estimates must show that dose rates do not exceed 7.5 micro Sv / h outside any shielded enclosure. In all cases, all the relevant exposure categories (effective dose, equivalent dose [extremities, skin, eyes]) must be given as well as measurements or estimates of annual exposures in all relevant categories to employees, other persons and members of the public. Consent will not be granted if HSE or ONR do not consider these ALARP.
The subject of this blog is the bolded text above. And whilst we acknowledge that this is ONR guidance and not HSE, the fact that patients are mentioned in the above text leads us to believe that the wording for HSE will be identical, unless changed in the next few weeks / months. Also HSE and ONR are mentioned in the above text (regarding ALARP) so this also leads us to believe that the text will be in the same in the HSE guidance.
What does Ionactive have an issue with?
'Dose rate' sounds generic but has a specific definition in IRR17 (more of that in a moment). The issue is that if there were a requirement (regulatory demand) that in any moment in time dose rates around a radiotherapy cancer treatment facility must be < 7.5 micro Sv/h, then there would be a whole load of treatment facilities around the UK which do not meet this. This is despite the fact that long proven analyses of such facilities show that exposures to staff (not involved in radiotherapy), and patients and visitors (not undergoing treatment) are low and in all cases substantially < 300 micro Sv/year (whole body dose) to critical persons.
Ionactive contention here is that 'dose rates' in the above ONR guidance are not defined. It is vitally important that they are defined for the medical sector. A simple improvement to this resource would be to state that all terms used have the meaning specified in IRR17 (2) - Interpretation of the legislation.
In the next section of this blog resource we will summarise 'dose rate' in the UK with respect to IRR17.
IRR17 dose rates (a primer)
This should be simple (and in reality it is), but it is worth analysing this in some detail.
Dose rate (UK)
Dose rate in the UK is defined in IRR17 as ‘in relation to a place, the rate at which a person or part of a person would receive a dose of ionising radiation from external radiation if that person were at that place, being a dose rate at that place averaged over one minute’. This can be found here: IRR17 (2) - Interpretation.
This definition can be usefully used if the dose rate at any point at any moment of time is brief (and significantly less than one minute), and so averaging over the minute is useful. An example might be monitoring the dose rate at the shielded curtain entrance or exit of an airport security system where the dose rate increases for a second or two as the baggage moves through the curtain, before returning to background levels. These peaks might occur a few times a minute, but analysis (and measurement) shows that for most of the time background dose rate exists. [In this airport security unit example we assume that dose rates are measured very close to the curtain, in reality dose rates in positions where passengers or airport security staff can stand will be very close to background]. This situation is depicted in the graphic below which is taken from our online Radiation Safety Awareness: X-ray security screening systems for freight, cargo and aviation course.
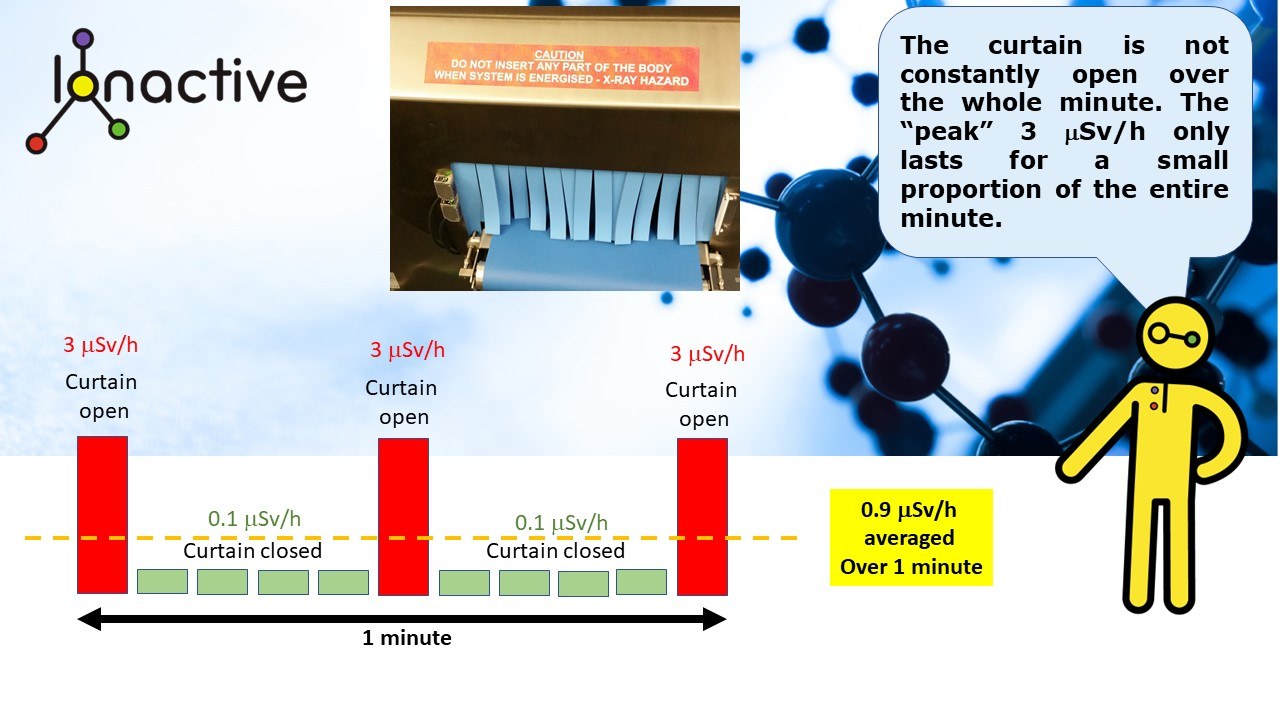
Short duration peak dose rates over 1 minute (x-ray screening unit)
IDR Instantaneous dose rate
IDR is not a specific term recognised in IRR17, but is used practically to mean a dose rate recorded at a moment in time. This dose rate may then be used in dose averaging calculations (such as micro Sv-in-any-one-hour or weekly / monthly / annual dose predictions). IDR and the definition of dose rate means, that in certain calculations, there may be double averaging taking place. This may be the case where the source of radiation is constantly moving in time. Whilst static dose rates are often taken during critical examinations (so worse case), averaging can be legitimately used when a conventional radiotheraohy linac bunker (shielded treatment room) is running VMAT arcs (radiation beam is constantly moving). However, it is Ionactive experience that most bunker calculations are based on static measurements with the beam constant at a specified gantry angle – this can lead to over design of the shielding in both IDR and time average dose rate conditions. As we will see below, a “headline” dose rate of > 7.5 micro Sv/h, as measured at an instant of time, may be completely unrepresentative of the maximum possible exposure that could be received by a person standing at that position for 1 hour.
Derived exposures may consider occupancy (i.e. the amount of time a critical person is in the area, in any one hour). In addition, the position of the beam is important – in an arc the beam is moving, for a simplification we can assume that the beam will be pointing 25% at 0, 90, 180, and 270 degrees. So a critical person standing close to a primary shielding barrier will only experience significantly increased dose rates above background for 25% of the total time of the exposure.
For now, assume a static beam and a critical person (outside the treatment room) is at 100% occupancy for 1 hour. Assume that four treatments take place in one hour (about the maximum credible when considering patient setup time). Assume that each treatment is 2 minutes duration, so that the 'beam on' time is 8 minutes in the hour. This means that for 52 minutes of each hour the dose rate to the critical person is background (assume this is 0.1 micro Sv/h). Let’s suppose that the IDR measured on a radiation monitor is a maximum of 12 micro Sv/h. This means that the maximum exposure to the critical person in the hour will be 1.7 micro-Sv-in-any-one-hour. Without considering occupancy or beam direction (both of which are extremely important), you can see how much lower the derived exposure per hour is as compared to the IDR dose rate measured at an instant. When gantry angle and occupancy is taken into account the exposure potential per hour drops to near background (more so if an arc – moving beam – is considered). This analysis alone shows that the ONR (and likely HSE) guidance should carefully define what it means by dose rate. Simple stating ‘dose rates do not exceed 7.5 micro Sv/h outside any shielded enclosure’ is a gross simplification and this must be challenged.
If an 'arc' treatment is being performed (more usual nowadays), then it is quite possible that only one "arc" will be detectable at a given measurement position in any one minute. If this is the case then someone standing at the primary wall would detect an IDR (e.g. starting at their head) which would rapidly move down the body and disappear near the feet (this could be the other way around if rotation is in the opposite direction). Suppose the IDR measurable at the trunk position is 12 micro Sv/h and this is detectable as it moves for 3 seconds, then the literal definition of dose rate could be used (i.e. average over one minute). Under this definition, the IDR was background (0.1 micro Sv/h) for 57 seconds and 12 micro Sv/h for 3 seconds). So the dose rate recorded would be: 0.7 micro Sv/h (as defined). This analysis is before considering any occupancy. It shows that with moving radiation beams the actual definition of dose rate is even more crucial in order to evaluate true exposure potential and to avoid over shielding.
Controlled Areas
There are a number of conditions / situations where a radiation controlled area can be defined in the UK. A common one is ‘where special procedures are required to restrict significant exposure or limit the probability of a radiation accident’. Another condition is where anyone working in the area is likely to receive more than 6mSv/year effective dose, 15mSv equivalent dose to the lens of eye or 150mSv equivalent dose to the skin and extremities (hands and feet). These conditions are found in IRR17 (IRR17 (17) - Designation of controlled or supervised areas) and consider routine occupational exposure and reasonably foreseeable radiation accidents.
The Approved Code of Practice (ACoP) to IRR17 has legal significance and goes further suggesting that a ‘controlled area is required where the external dose rate in the area exceeds 7.5 µSv per hour when averaged over the working day’. There are some slight differences related to certain practices, so open site radiography for example will use averaging over one minute to set the controlled area designation.
The IRR17 ACoP guidance also states what might be considered an upper level of acceptable IDR even if it can be shown that radiation levels at the protected perimeter are < 7.5 micro Sv/h when averaged over an 8-hour working day. This upper level is set at 100 micro Sv/h IDR. This could be further interpreted as: No controlled area is required where instantaneous dose rate (IDR) exceeds 7.5 micro Sv/h, where the dose rate averaged over minute is <7.5 micro Sv/h, as long as the IDR dose rate does not exceed 100 micro Sv/h. In this case it would be expected that those untrained in radiation safety and members of the public do not have unrestricted access to the area.
The point here is that the simple expression in the noted ONR guidance (... < 7.5 micro Sv/h... ) is not that helpful and does not take into account how dose rate can be interpreted in the legislation. Considering the above analysis, and the example given for a critical person outside a radiotherapy primary shield (where IDR was 12 micro Sv/h), no controlled area would be required in these specific circumstances. In addition, subject to shielding analysis, it could also be shown that ALARP is also achieved. This last point should be considered with care - it might be valid for a current facility, or one that has been upgraded with a newer linac, but the ALARP test may not pass (or be as demonstrable), if this was a band new facility currently on the drawing board.
Ionactive comment
We hope that by the time the HSE consent guidance has formally been released, the issue of dose rate will have been helpfully defined. If nothing else, reference should be made to the IRR 17 definitions in IRR17 (2) - Interpretation and controlled areas, IRR17 (17) - Designation of controlled or supervised areas.
In many cases, specifically related to radiotherapy bunkers (shielded treatment rooms), an IDR of < 7.5 micro Sv/h is achieved outside primary shields (regardless of beam direction, occupancy and similar). However, there is no reason why this has to be the case and achieving this "goal" should not be used as a basis for shielding design, when it can be shown that time average dose rates (micro-Sv-in-any-one-hour) can be used to show that maximum exposures in any one hour are essentially trivial and very close to background.
Mark Ramsay
Radiation Protection Adviser
Ionactive Consulting Limited - July 2023