

A dose rate of 1 micro Sv/h. A magic line or a bit of a nonsense?
Published: Aug 26, 2024
Updated 19 May 2025
This blog article now contains our newly released radiation protection widget - True whole body dose rate from an x-ray cabinet apparent radiation "leak" widget (opens in a new tab). Play with the widget located directly in this blog article, and if you want more information on what it does then visit the included link to its own page.
Outline
Often an x-ray machine (cabinet) manufacturer will state their equipment meets a limit of < 1 micro Sv/h (on the surface, at 10cm from the surface or at some other distance). In Ionactive experience this has often been treated as a ‘legal limit’ by the supplier or end user – so much so that some RPAs (e.g. for airports and similar) have insisted that dose rates exceeding this level must be reduced to the ‘safe’ level. Clearly ALARP (as low as reasonably practicable) comes into play, but what and where is the actual potential radiation hazard? This blog article investigates where 1 micro Sv/h arises from, where around the world this may differ (e.g. US cabinet x-ray standards), how it is (or should be) interpreted, and where (in the UK) it is completely unusable as an IRR17 exemption from notification (Schedule 1).
Prelim
Here are a few randomly selected extracts from radiation safety data sheets / operating manuals for cabinet x-ray systems available around the world (these examples are taken for x-ray units that can be supplied into the UK).

Examples of <1 micro Sv/h for cabinet x-ray systems
There are plenty more examples, the above is just a taster. In the US you might see words to the effect of ‘does not exceed an exposure of 5 micro Sv in one hour at any point 5cm from the surface’ (converted to SI units - actually written as 0.5 milliroentgens), we will look at this later. There are also a few examples where much lower emission levels are specified, for example one x-ray company from Türkiye states 'X-ray Leakage: <0,05 μGy' (which is practically saying emission levels are no greater than typical background).
So where has the magic 1 micro Sv/h [1 μSv/h] (at some distance) come from, and where does it appear in the UK Ionising Radiations Regulations 2017 (IRR17)?
Derivation of 1 micro Sv/h at 10 cm from the surface
From a European perspective, a common recognised ‘standard’ for an acceptable dose rate outside areas that are uncontrolled (for the purposes of restriction of exposure from x-ray devices) is <1 micro Sv/h (at 10 cm from any accessible surface). As will be noted later, it is acceptable to time average this value such that the numerical value reflects the quantity ‘<1 micro Sv-in-any-one-minute’, or ‘<1 micro Sv-in-any-one-hour’. Therefore it is not unusual that an instantaneous dose rates (IDR) exceeds the value 1 micro Sv/h (whereas time averaged dose rates do not). The derivation of the 1 micro Sv/h ‘standard’ is not entirely transparent but is best referenced thus.
First consider - Article 26 of the COUNCIL DIRECTIVE 2013/59/EURATOM of 5 December 2013 'laying down basic safety standards for protection against the dangers arising from exposure to ionising radiation'. Whilst the UK has now gone through Brexit, DIRECTIVE 2013/59/EURATOM was the legal driver for creating IRR17 and so IRR17 is compatible with the Directive today regardless. Note that the former UK IRR99 regulations also contained the same '<1 micro Sv/h ...', this being driven by the former 96/29/Euratom Directive.
In the referenced Directive, the <1 micro Sv/h ‘standard’ is commonly used to provide exemption from (most) regulation by the member states (Article 26-d-I, ii – “exemption from notification”). A graphic with the relevant text highlighted is shown below.

Article 26-d-I, ii – “exemption from notification”
Whilst exemption is not always available (e.g. there is no exemption available in the UK – more of that in a moment), the clear intention is that at these levels of likely exposure the risks from radiation are low and are of negligible concern (i.e. meets the principle of ALARA internationally and As Low as Reasonably Practicable - ALARP - in the UK). With respect to cumulative annual exposures, the intention might be to treat the operator as a member of the public. In the UK the dose limit for a member of the public (or other person not engaged in work with ionising radiation - 'other persons') is 1mSv effective dose annually, with a further dose constraint of 300 micro Sv for a single practice.
[Ionactive comment: the above dose constraint will illustrate the problem with over estimating exposures based on a dose rate of up to 1 micro Sv/h. If you do not account for geometry, what part of the person is exposed, where the person is in relation to the x-ray unit, how much of the working year they are near the x-ray machine etc, then it might be assumed the constraint could be exceed in 300 hours (about 15% of a working year). This is clearly a nonsense but we have seen plenty of examples of just this type of assessment.]
The distance ‘at 10cm’ is written specifically into the directive.
[Ionactive comment: since monitor response will vary, and taking account of the technique used by those monitoring, where practicable the measurement is best made at the surface initially (or at least as well as taking at 10cm).]
Also note the Directive uses the term 'accessible surface'. Does this mean literally (i.e. at the top of a tall x-ray unit accessible via a ladder), or can reasonably practicable be applied (i.e. monitoring where persons are likely to be located most of the time)?

Determining <1 micro Sv/h 'where accessible'
Outside of the EU, and this is the case with the UK now, the same values can be found in higher level IAEA documentation. For example, the following features in section I3ci from Schedule 1 of ‘GSR Part 3 Radiation Protection and Safety of Radiation Sources - IAEA ( 2014)', noting that this IAEA publication (derived from the recommendations of ICRP 103), is the current top level world wide document on such matters (for member states of IAEA).

IAEA GSR Part 3 - Exemption
Note carefully the wording. For x-ray equipment [radiation generators] (not including cathode ray tubes for display), the exemption for x-ray equipment is qualified by “type approved by the competent authority” (EU Directive) or “Radiation generators of a type approved by the regulatory body” (IAEA). So this means that the exemption is optional based on the member states preference to provide type approval for x-ray equipment (and for this blog we mean type approval of x-ray cabinet systems).
Now let us turn to the UK IRR17. The above wording (from the Directive / IAEA) appears in Schedule 1 of IRR17 in the following form (Schedule 1, work not required to be notified under regulation 5). [Ionactive comment: If you would like a full set of guidance on IRR17 - then head over to: Ionactive guide to the Ionising Radiations Regulations 2017 (IRR17).]

IRR17 - Schedule 1 (work not required to be notified)
As you see a similar qualifier appears – “the apparatus is of a type approved by the Executive”. The executive is the UK Health and Safety Executive (HSE). There are no type approvals for x-ray equipment in the UK, there have never been, and there never will be. This means that for our cabinet x-ray units under consideration in this blog, Schedule 1 is completely irrelevant and there is no exemption from notification. The use of x-ray units require a registration under IRR17 (or potentially a consent if the work is industrial radiography and the enclosure can be easily entered, or if the unit is used for industrial irradiation). Note that registrations and consents in the UK are per legal entity, not per x-ray unit or premises.
This is an important finding - since for years Ionactive has been aware of x-ray unit supply companies, end users (and some RPAs) who read Schedule 1 of IRR17 (or IRR99 before) and assume the x-ray equipment is exempt in the UK because the standard has been met.
So – the magic < 1 micro Sv/h has no official regulatory purpose in the UK. Is it just a magic line in the sand?
Why do we expect <1 micro Sv/h in the UK when conducting critical examinations?
The <1 micro Sv/h ‘standard’ is recognised around much of the world (for x-ray cabinet systems). The fact that it can be used to exempt member states from significant regulation of x-ray units (but not in the UK), implies that levels below 1 micro Sv/h are approaching background (true with ‘sensible hat on’ – see next section for some analysis of this).
In fact there are companies in the UK who manufacture x-ray cabinet equipment for a worldwide market which includes the US. Such equipment in the US must comply with the cabinet x-ray standard : Cabinet X-Ray Systems (Closed X-Ray Systems) [21CFR1020.40]. In this standard it is stated that: ‘external radiation emission from a cabinet x-ray system [will not] exceed an exposure of 0.5 milliroentgens in one hour at any point five centimetres outside the external surface’. For our purposes this is translated as < 5 micro-Sv-in-any-one-hour at 5cm from the surface. Despite this emission limit the UK manufacturer ensures that the US machines meet <1 micro Sv/h (at 10 cm) as well as < 5 micro Sv/h at 5cm so that the unit can be sold anywhere in the world.
Note that the US standard is specifically time averaged over 1 hour, there is no specific Instantaneous Dose Rate (IDR) limit. In the UK dose rate is defined as a dose rate at point which is averaged over 1 minute (IRR17). It follows (with sensible hat on) that the measurement taken in the UK could literally be an IDR (i.e. taken over a second or two), or might be the dose rate averaged over 1 minute. This concept is useful for dose rate measurements at the infeed and outfeed of certain x-ray cabinets (generally fitted with shielding curtains). However, Ionactive has experienced occasions where a blip of 1.3 micro Sv/h (taken at an instance) has caused a site to shut the x-ray unit down for ‘safety reasons’. Despite this, most RPAs and users accept that on most occasions dose rate can be averaged over an hour to show that the time average dose rate is < 1 micro-Sv-in-any-one-hour. This is following the US practice (but at lower exposure levels) and is essential for certain applications (such as cargo / freight systems screening large objects causing significant shielding curtain displacements several times a minute).
Interestingly, the prescriptive x-ray safety warning signs required by 21CFR1020.40 are also generally used for all equipment sold anywhere in the world.
Overall, for many cases in the UK , the < 1 micro Sv/h standard is often considered a legal safety limit. It is not a legal safety limit and to treat it as such can cause some interesting issues. We will now looks at some of these.
Some potential issues when aiming to measure <1 micro Sv/h around cabinet x-ray systems
IDR or time averaged
We introduced IDR (instantaneous dose rate) earlier in this article. If you have a completely contained x-ray cabinet, with an interlocked door and no possible access when x-rays are being generated (e.g. no shielding curtains / open ports etc), then a real time IDR is useful. By instantaneous we mean – take a reading, check you are happy with it and record the value. This should be all you need at the point of measure. [Ionactive comment – this is absolutely NOT the case for a large shielded facility containing a linac for cancer treatment, where the x-ray beam may be rotating around an axis. This has been discussed here 'New UK IRR17 consent - dose rate and accelerators', and we will revisit this further another day].
Where there is potential access near to the infeed / outfeed shielded curtains, then IDR alone may significantly exaggerated the true potential radiation exposure in that area. The following graphic, taken from Ionactive online training courses, demonstrates the issue.
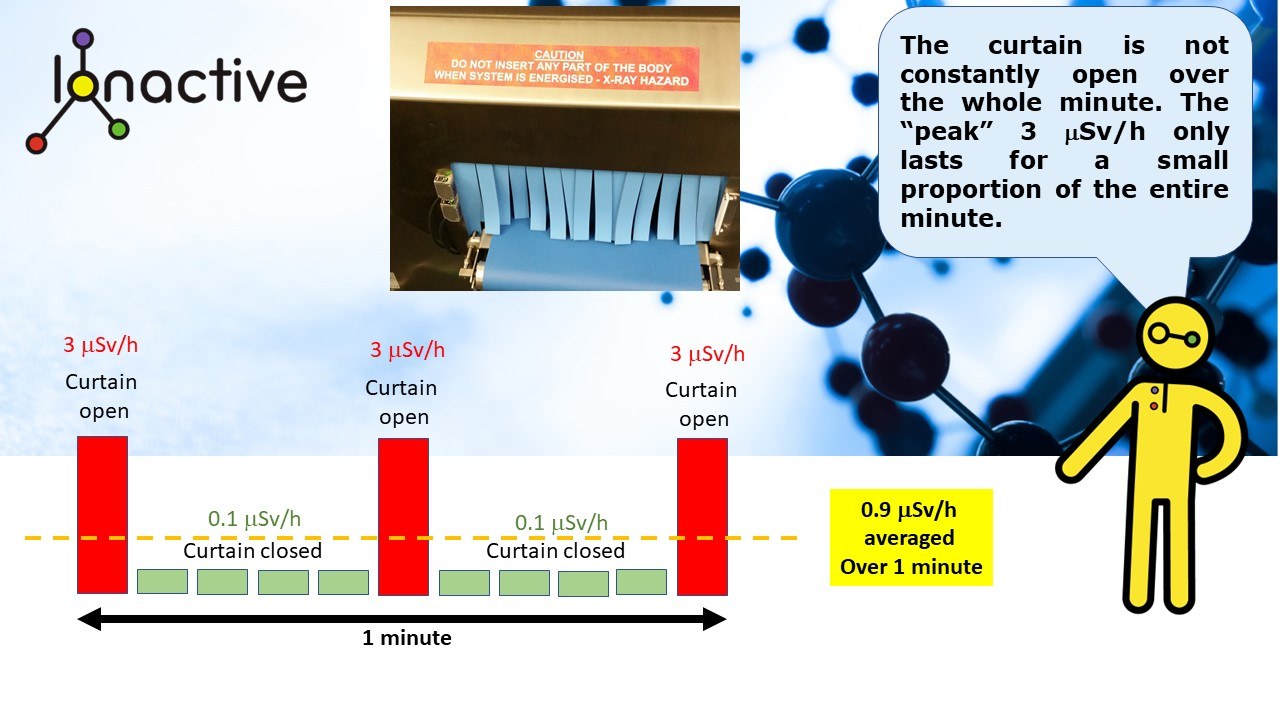
IDR dose rates and Time average dose rates (over one minute)
Here you see that the headline IDR is 3 micro Sv/h, but the time average dose rate over a minute is 0.9 micro Sv/h. If you just consider 3 micro Sv/h alone you might assume that the magic 1 micro Sv/h is exceeded.
Overall - the headline “value” is less important than the context in which is it occurs and is measured.
What / who is being exposed?
Consider the following food x-ray screening system. A conveyor runs directly up to the infeed x-ray curtains / tunnel (indicated by yellow arrow). A conveyor also runs directly from the outfeed tunnel of the x-ray unit (not shown). Therefore, if a radiation IDR measurement is taken just at the infeed / outfeed curtain surface, it cannot indicate whole body exposure potential at that point. [Ionactive comment – it might infer equivalent dose to the hands which is considered in the next section].

Dose rate measurement (whole body exposure estimate) - realistic position
The point is – when undertaking a radiation survey, perhaps during a critical examination around an x-ray cabinet system, the radiological performance is best measured by taking measurements in areas where someone might be present. In the above diagram potential whole body exposure is being measured at the nearest realistic approach to the infeed shielding curtains (orange arrow).
If only headline dose rates (typically IDR) are taken (yellow arrow), particularly attempting to measure the highest possible IDR, then this can completely over exaggerate the actual radiation exposures possible. It’s as if the higher radiation dose rates might float around and then impact on a person located near by (obviously completely not the case!). There is nothing wrong taking such measurements as part of an investigation for a risk assessment, for example assessing the consequence of a shielding curtain failure (by carefully monitoring either side of the curtain). The important point is that should the curtain fail, what is the whole body dose rate where someone can be exposed?
What part of the body is being exposed / what dosimetric quantity is measured?
The above mentioned EU directive uses the term dose rate. However, the IAEA standard goes further and uses ‘ambient dose equivalent rates’ . Ambient dose equivalent is an ‘operational quantity’ and is often used as an approximation of effective (whole body) dose (generally over estimating rather than underestimating). Overall the intention is to base the magic <1 micro Sv/h on ‘whole body dose’ measurements. This might make sense if the trunk of the body is fully exposed to a large area x-ray leak from the end of a poorly shielded x-ray cabinet (this assumes there is no infeed / outfeed conveyor in the way). However, often when making x-ray leakage measurements, dose rates that approach 1 micro Sv/h (at 10cm or at the surface) are from small discrete areas of the x-ray cabinet. An example is shown below - a tight corner in the exterior of the x-ray cabinet. Notwithstanding any additional debate on the size of the monitoring probe required to take such measurements, in the example illustrated - what part of the body is going to be exposed?

What part of the body can be exposed to a level > 1 micro Sv/h ?
It is impossible to receive a whole body dose from x-ray leakage at this point (note the yellow arrow). Even if an operator, for whatever reason, was to climb on to this area and settle their body tight into the corner (!), which part of the trunk of the body is exposed? Top, back, left, right? A more realistic exposure potential is placing their hand (s) into this area (for some reason). However, we are now moving away from the whole concept of the magic < 1 micro Sv/h – since an exposure to the fingers will be an equivalent dose. The UK equivalent dose limit to the fingers (extremity) for someone not involved with work with ionising radiation (generally denoted other persons) is 50 mSv per year. This limit has been chosen as it is the lowest limit to be applied to this part of the body (the legal limit for persons working with ionising radiation is 500 mSv when over the age of 18 years). Imagine an operator who, for whatever reason, leans against the machine and places their hand in this position (see above) for 1 minute per hour, 8 hours a day, 5 days per week, 50 weeks a year. At a measured dose rate of 1 micro Sv/h, the accrued dose over the year would be 2000 micro Sv (2 mSv) which is 4% of the annual extremity dose (50mSv) noted above. Ionactive visits such work environments several times each month and observations are that operators don’t work this way – the above calculations are ridiculously pessimistic, but even so – it is still a tiny fraction of the dose limit. In addition, the likely whole body radiation exposure from this scenario will not be measurable or calculable above background.
Now ask yourself this – what difference would it make if the headline dose rate value at this location was actually 1.5 micro Sv/h in the corner? Have you crossed the magic < 1 micro Sv/h line – have you crossed from safe to danger? Ionactive agrees that lines in the sand can be useful and simple to use – but in the above scenario they do not represent ALARP, rather they show a misunderstanding of potential exposures (and where those exposures may occur). And remember - this is not about legal limits, it is a standard derived from an intention to simplify radiation safety regulation, which does not apply in the UK (i.e. at least a registration from HSE is required for use of radiation generators including x-ray units).
True whole body dose rate from an x-ray cabinet apparent radiation "leak" widget
(New from 19 May 2025).
As a bit of a diversion try out the new Ionactive radiation protection widget below.
If you would like a more in-depth explanation of this widget then please head over to: True whole body dose rate from an x-ray cabinet apparent radiation "leak" widget.
How big is the exposure area?
This follows on from the previous blog section before the widget interlude. Imagine a large airport checked baggage screening system where the airport RPA has discovered a small x-ray “leak”. It happens to be a small short path covering an area of ‘1 pence” (20mm diameter). The measurements are 2 micro Sv/h at the surface and 1.3 micro Sv/h at 10 cm from the surface. Measurements are taken using a RadEye G-10 radiation monitor. The RPA for the x-ray unit is called in to have a look at the ‘leak’. They have a Mini 900 D dose rate monitor and a Mini 44A CPS scintillation monitor. Access to the area of concern is via a ladder.

Monitoring the '1 penny' x-ray leak on top of the x-ray unit
The supplier RPA first attempts to measure the spot using the 900D monitor – but the area of leakage is a virtual pinhole, the surface dose rate varies from 0.5 micro Sv/h to 1.8 micro Sv/h depending on the exact orientation of the probe. The area of leakage is easier to detect using the 44A probe which gives a good 300 CPS and associated noise. Returning to the 900 D monitor, the highest dose rates are then recorded as 1.9 micro Sv/h on the surface and 1.1 micro Sv/h at 10cm from the surface. Note – different monitors, different results.
We also note that the supplier RPA has to “hunt” for the hot spot. The RPA then uses a 451p ion chamber monitor (not shown in the picture) over the spot (this monitor being energy independent of the leakage x-ray energy). Dose rates at the surface are measured at 0.1 micro Sv/h.
The airport RPA states the monitor is inadequate since the 451p has a large detector area and the x-ray leak will not completely fill the chamber- so the monitor will under-read.
The x-ray equipment supplier RPA responds stating that this is the whole point of the ion chamber measurement - the “leak” can neither fill the detector volume, or interact with the trunk of the body to give a whole body effective (or ambient dose equivalent).
Given the magnitudes of the IDR dose rates recorded, the area extent, and the location (right on top of the x-ray unit away from anyone), the supplier RPA suggests that the area of concern is noted for the record, but advises there is negligible radiation risk present. The airport RPA disagrees and wants the area ‘leaded’, and since the customer is always right, the x-ray equipment provider dutifully places some lead under the outer cover to bring dose rates down to << 1 micro Sv/h (now at the surface!).
Is the above scenario ALARP? Or is there an obsession over the magic < 1 micro Sv/h? Is everyone safer now that the x-ray ‘leak’ has been mitigated to << 1 micro Sv/h (at the surface). Who has benefited, or will benefit in the future? Whilst it might be argued that the time in effort and materials to place additional lead over the area was not excessive, others might counter-argue that a ‘dose assessment’ has been missed, and instead reliance on being the ‘safe side' of the magic line has been given more weight then it deserves. ALARP does not mean as low as possible. For this example we deliberately use a ladder for access - probably in reality a better / safer access method might be used.
Is occupancy considered?
We discussed occupancy earlier in this article (operator placing their hand into a corner area of an x-ray unit for 1 minute every working hour of the year). Now apply occupancy to the scenario just discussed above (airport security machine). Let’s assume that the additional lead shielding was not completed. How often will someone come into contact with the ‘hot spot’. A minute or two a year whilst an engineer changes a light bulb in the ceiling above the x-ray unit? Even if this were so, what part of the engineer is going to be exposed to this hot spot, and will it be the same part each time? As also noted earlier, the airport engineer cannot receive a whole body dose from the x-ray 'leak' described.
Occupancy for these scenarios is not normally considered – but in some cases it should be! [Ionactive comment: as mentioned before, occupancy is very much a consideration in medical uses of radiation particularly with linac accelerators where relative high IDR (say 10 micro Sv/h) are present for short periods several times in a single hour].
Even if occupancy is not formally assessed or calculated, the 'sensible hat' can be worn and not even a back of an envelope calculation is required to show that potential radiation exposures are trivial and not materially measurable (or calculable) above background.
So what are we saying exactly?
It is important to note that this is an Ionactive blog post and is not official guidance. We use this area of our website to discuss radiation protection, asking questions you might not have considered before. We like to be constructively provocative 😊.
We are not suggesting the <1 micro Sv/h (at some distance) is a nonsense, well not really (!). But we do question how it is often used. In this article we have discussed:
- Where the <1 micro Sv/h (at 10cm) has come from.
- How its purpose (to simplify or reduce regulation) cannot be applied in the UK (no type approval).
- How it might be used as a surrogate for 'safe radiation exposure', if you are the safe side of the magic line.
- It is not a legal (dose rate) limit (at least not in the UK).
- How reducing all radiation exposures, regardless of where they are, to < 1 micro Sv/h (at some distance) is not ALARP (in all cases).
- How time averaging, and acknowledging the IRR17 definition of dose rate, is essential in many cases to actually comply with this standard (e.g. infeed and outfeed tunnels protected by lead shielding curtains with higher IDR above 1 micro Sv/h).
- How in almost all cases it is unlikely, if not near impossible, to receive a whole body dose from any dose rate (hot spot) that is measurable above background.
It is also useful to note that much of the time we (Ionactive) never measure IDR dose rates anywhere near 1 micro Sv/h (and where we do it is usually in the region of infeed / outfeed areas as already discussed). So generally there is no problem complying with this magic line, as long as you accept that to exceed it does not automatically bring you into the danger zone.
Mark Ramsay
Radiation Protection Adviser
Chartered Radiation Protection professional
(c) Ionactive Consulting Limited - August 2024